https://gut.bmj.com/content/69/9/1592
Abstract
Objective Treatment options for non-hospitalised patients with coronavirus disease 2019 (COVID-19) to reduce morbidity, mortality and spread of the disease are an urgent global need. The over-the-counter histamine-2 receptor antagonist famotidine is a putative therapy for COVID-19. We quantitively assessed longitudinal changes in patient reported outcome measures in non-hospitalised patients with COVID-19 who self-administered high-dose famotidine orally.
Design Patients were enrolled consecutively after signing written informed consent. Data on demographics, COVID-19 diagnosis, famotidine use, drug-related side effects, temperature measurements, oxygen saturations and symptom scores were obtained using questionnaires and telephone interviews. Based on a National Institute of Health (NIH)-endorsed Protocol to research Patient Experience of COVID-19, we collected longitudinal severity scores of five symptoms (cough, shortness of breath, fatigue, headaches and anosmia) and general unwellness on a four-point ordinal scale modelled on performance status scoring. All data are reported at the patient level. Longitudinal combined normalised symptom scores were statistically compared.
Results Ten consecutive patients with COVID-19 who self-administered high-dose oral famotidine were identified. The most frequently used famotidine regimen was 80 mg three times daily (n=6) for a median of 11 days (range: 5–21 days). Famotidine was well tolerated. All patients reported marked improvements of disease related symptoms after starting famotidine. The combined symptom score improved significantly within 24 hours of starting famotidine and peripheral oxygen saturation (n=2) and device recorded activity (n=1) increased.
Conclusions The results of this case series suggest that high-dose oral famotidine is well tolerated and associated with improved patient-reported outcomes in non-hospitalised patients with COVID-19.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
COVID-19 is a global pandemic caused by the severe acute respiratory syndrome coronavirus 2. COVID-19 is highly contagious and causes a spectrum of disorders ranging from relatively mild symptoms to life-threatening conditions. Medical therapies that interrupt COVID-19 progression in non-hospitalised symptomatic patients are therefore highly sought.
What are the new findings?
We devised a method to quantitatively follow six common symptoms in non-hospitalised patients with COVID-19 over the course of their illness. The individually normalised patient symptoms revealed that the self-administration of the histamine-2 receptor antagonist famotidine is associated with symptomatic improvements in a case series of 10 consecutive patients.
How might it impact on clinical practice in the foreseeable future?
Our findings support the rigorous evaluation of famotidine as a potential therapy and of the use of symptom tracking for non-hospitalised patients with COVID-19.
Introduction
Management of patients with coronavirus disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), poses a major challenge to the biomedical community, governments and global population. Currently, most research focuses on vaccine development or pharmacological treatment strategies for hospitalised patients with COVID-19.1 However, to reduce global morbidity and mortality, effective treatment strategies for non-hospitalised patients are required.
Famotidine may be a candidate medication for this. Famotidine is a histamine-2 receptor antagonist, widely available over the counter at low cost, does not interact with other medications and has been safely used for suppression of gastric acid production over a wide range of oral doses from 20 mg once daily to 160 mg four times daily.2 In computer simulations, famotidine was identified as a potential inhibitor of the 3-chymotrypsin-like protease,3 and this and other potential mechanisms of action for famotidine in COVID-19 are an area of current research. In a propensity score matched retrospective cohort study a significantly reduced risk for death or intubation (adjusted HR 0.43, 95% CI 0.21 to 0.88) was identified for patients with COVID-19 who were incidentally taking famotidine before or at the point of hospital admission.4
The incentive for the retrospective cohort study were the unexpected positive results from a group of 10 patients who took famotidine following onset of symptoms for COVID-19. Here, we summarise this series of 10 patients with COVID-19 who self-medicated with famotidine as outpatients. The patient-reported demographics, clinical course, drug tolerability and longitudinal symptom scores are provided.
Methods
Consecutive patients were enrolled in this study after signing written informed consent for study participation and for deidentified data being reported in a published case series. No participant was excluded. Data were collected by two telephone interviews and two written questionnaires. Information on patient demographics, comorbidities, COVID-19 test results, famotidine use, drug-related side effects, temperature measurements, oxygen saturations and symptom scores were obtained. We collected longitudinal severity scores on five symptoms (cough, shortness of breath, fatigue, headaches and anosmia), based on an NIH endorsed Protocol to research Patient Experience of COVID-19, in addition to general unwellness.5 Symptom scores were retrospectively provided by patients on an ordinal scale: 1=not affected, 2=little affected, 3=affected and 4=severely affected. This four-point scale was based on performance status scoring in patients with cancer who are systemically affected by illness or treatment. We adapted the first four scale points of the Eastern Cooperative Oncology Group performance status (ECOG PS) scale6 and provided explanatory text to the patients as part of the symptom questionnaire. We chose only those scale points of the ECOG PS as measures of grades of severity that are relevant to a severity of COVID-19 illness that does not require hospitalisation. The relevant sections of the questionnaire with the introduction to the scale and scoring system were provided to the participants and are included in the online supplementary methods section. Longitudinal symptom scores for the time prior to the COVID-19 illness (baseline, B), the day before starting famotidine (day −1), the day famotidine was started (day 0) and days 1, 2, 7 and 14 after starting famotidine were recorded. Longitudinal temperature recordings, pulse oximetry and activity monitoring data were recorded when available.
Supplemental material
Results
Patient characteristics
Ten individuals with the clinical diagnosis of COVID-19 who self-medicated with high dose oral famotidine were identified. Eight patients were from New York State, one from New Jersey and one from Sweden. The characteristics of all study participants are summarised in table 1. The study participants were diverse with regard to known risk factors for severity of COVID-19 illness: age, sex, ethnicity and body mass index (BMI).7 Seven patients had positive PCR-based diagnoses from nasal swabs for SARS-CoV-2, two patients had positive serological tests for antibodies directed against the virus and one patient had a clinical diagnosis without molecular confirmation (table 1). All started taking famotidine while feeling unwell with COVID-19. The most commonly used dose was 80 mg oral famotidine three times daily (n=6), and the dose ranged from 20 mg three times daily to 80 mg three times daily. Median duration of famotidine self-administration was 11 days (range 5–21 days). The time period between onset of symptoms and starting treatment differed widely between patients, ranging from 2 days to 26 days (figure 1).

Symptomatic days before famotidine start. The durations of symptoms prior to starting famotidine are displayed in ascending order for individual patients.
Patient characteristics
Patient-reported toxicity
Seven patients did not experience any adverse events. One patient reported grade 1 dizziness and very occasional perceptions of a racing heartbeat. Another patient experienced grade 1 dizziness, dry skin and insomnia. A third patient reported grade 1 gastroenterological symptoms and temporary forgetfulness (table 1). Other than forgetfulness, all of these side effects are listed in the prescription information for famotidine,2 and all side effects resolved on discontinuation of famotidine.
Patient-reported outcomes and symptoms
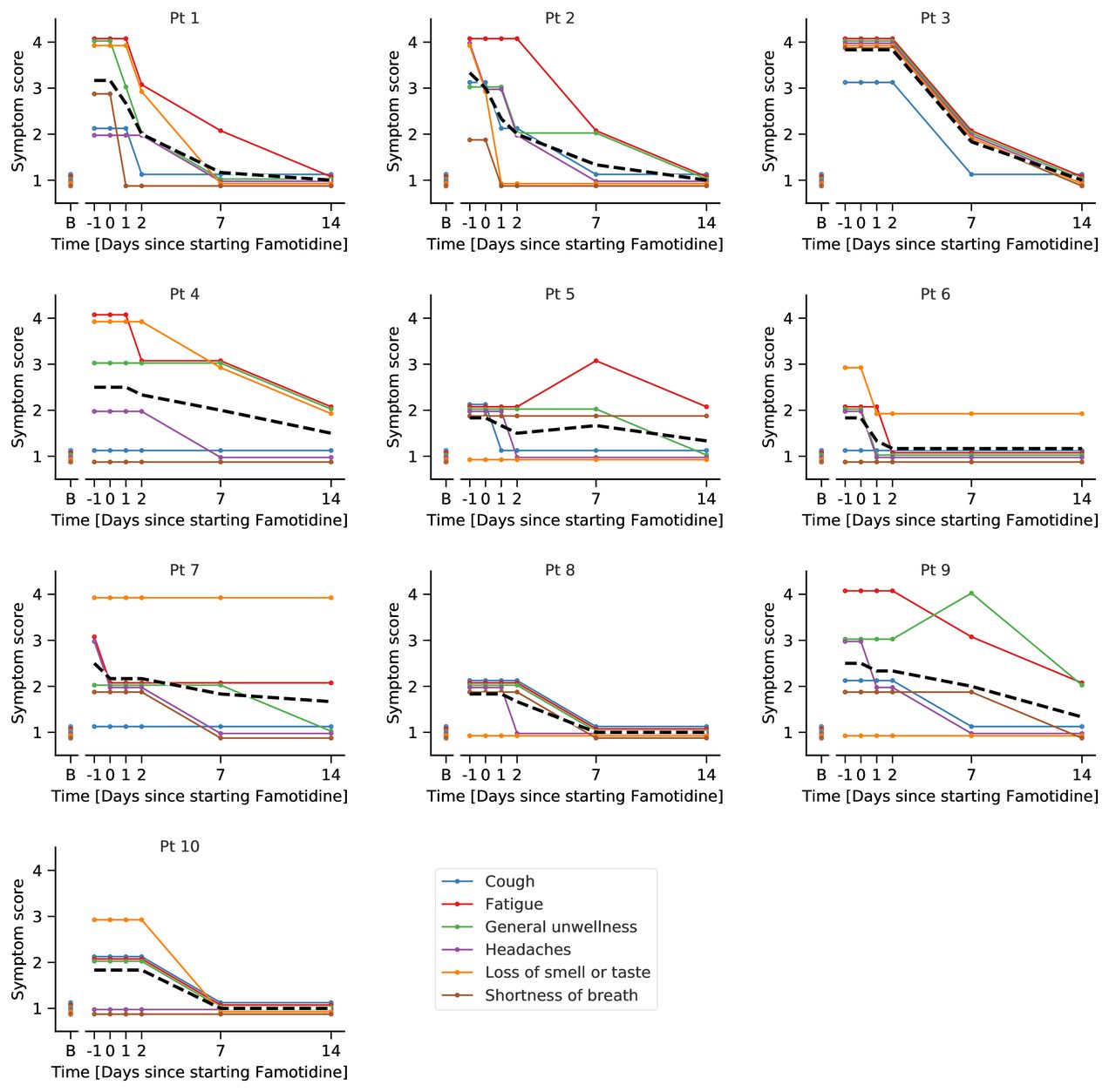
No hospitalisations were reported by any of the participants, and at the point of submission of this manuscript, patients reported feeling fully recovered apart from persistent anosmia in two cases. All patients were asymptomatic prior to developing COVID-19. They all were affected by a wide range of symptoms when they were feeling worst, and this was comparable with how they felt on the day prior to starting famotidine. On starting famotidine, all patients reported improvement of symptoms within 24–48 hours (case synopses and figure 2). When we analysed the changes of the normalised total symptom score across all patients, we found no significant difference for the day before starting famotidine compared with the day of starting famotidine, but a significant improvement in the symptom score was reported within 24 hours of starting famotidine and symptoms continued to improve and nearly normalised to preillness levels at 14 days after first famotidine use (figure 3). The improvement of symptoms was across all categories, but airway-related symptoms such as cough and shortness of breath were reported to improve more rapidly than systemic symptoms such as fatigue (figure 2).

Patient level symptom scores. The longitudinal data for all reported symptoms are shown for individual patients. The mean is indicated as a dashed black line. The baseline scores are indicated adjacent to the y-axis. All patients reported baseline symptoms at 1. Colour-coded lines and dots for respective symptoms are ordered alphabetically and are slightly offset to avoid overlap. Day 0 indicates the day at which patients took the first dose of famotidine. Severity score: 1=not affected, 2=little affected, 3=affected, 4=severely affected. B, baseline; Pt, patient.

Normalised symptom scores of all patients. The mean longitudinal normalised symptom score for all patients is shown. The SE of the mean is indicated. Statistical comparisons by two-sided t-test in comparison with day 0, the day of starting famotidine. *P<0.05; ***p<0.001; ****p<0.0001. NS, not significant.
Individual case summaries
Patient 1 is a white woman in her 40s with a medical history of epilepsy for which she takes levetiracetam 1 g daily. She took famotidine 80 mg three times daily for 11 days starting 4 days after first experiencing symptoms of COVID-19. She reported feeling very unwell at this time point. Within 1 day of the first dose of famotidine, she noticed marked improvement of her shortness of breath. This improvement was matched by an increase in her home-monitored pulse oximetry measured oxygen saturation levels from 91%–95% to 97%–98% (figure 4A). She was febrile with a temperature of 37.8°C prior to starting famotidine and afebrile on day 7 of taking famotidine.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patient-level pulse oximetry and activity results. (A) The pulse oximetry data from two patients are displayed. (B–D) The device software provided display of weekly data relating to three metrices recorded using an Oura Ring are displayed for patient 8. The mean for each metric over the displayed period is indicated by a dashed line. Day 0 and week 0 represent the day and week of starting famotidine, respectively. Pt, patient.
Patient 2 is a Hispanic man in his 40s without pre-existing conditions. He took famotidine 80 mg three times daily for 11 days starting 8 days after first experiencing symptoms of COVID-19. He reported improvement of symptoms within 2 days of treatment. He was febrile with a temperature of 38.3°C prior to starting famotidine and afebrile on day 5 of taking famotidine.
Patient 3 is an Asian man in his 30s without pre-existing conditions. He took famotidine 80 mg three times daily for 7 days starting 9 days after first experiencing symptoms of COVID-19. He experienced severe shortness of breath prior to starting famotidine, and his dyspnoea and other symptoms improved by day 7. His home monitored oxygen saturation levels improved from 89% on day 2 of treatment to 96% on day 5 of treatment (figure 4A). He was febrile with a temperature of 38.9°C prior to starting famotidine and afebrile on day 5 of taking famotidine. He intermittently took paracetamol for fever during illness.
Patient 4 is a black woman in her 60s with a BMI of 38, positive smoking history and hypertension controlled by triple therapy. She took famotidine 50 mg three times daily for 12 days starting 10 days after first experiencing symptoms of COVID-19. She noticed improvement in muscle aches and chest tightness in addition to those recorded in figure 2.
Patient 5 is a white man in his 50s iswith hypertension and hyperlipidaemia, both treated with medications, and positive smoking history. He took famotidine 80 mg three times daily for 8 days starting 6 days after first experiencing symptoms of COVID-19. He described ongoing increase of fatigue for another 7 days after starting famotidine; the only patient to describe worsening of any symptoms during this treatment period. However, he noticed improvement in respiratory symptoms within 2 days of starting famotidine.
Patient 6 is a Hispanic woman in her 20s with no pre-existing conditions. She took famotidine 80 mg three times daily starting 9 days after first experiencing symptoms of COVID-19. She felt markedly better within 2 days of treatment but had mild dizziness and accelerated heart beats intermittently while taking famotidine.
Patient 7 is a black and Hispanic woman in her 20s with a BMI of 41 with no pre-existing conditions. She took famotidine 80 mg three times daily for 12 days starting 6 days after first experiencing symptoms of COVID-19. Within 1 week of treatment, she reported relief of most symptoms. She reported grade 1 dizziness, insomnia and dry skin concurrent with taking famotidine.
Patient 8 is a white man in his 70s with history of myocardial infarction, surgery for a benign pancreatic tumour, chronic pancreatitis and chronic back pain. His diagnosis is based on clinical symptoms and signs and being from a high prevalence location, with all family members being clinically affected by COVID-19. He took Famotidine 60 mg two times daily for 5 days starting 26 days after first experiencing symptoms of COVID-19. He reported a rapid improvement and being asymptomatic within 3 days of treatment. He routinely monitors his activity using an Oura Ring device and was able to provide readings on walking equivalence, calorie usage and activity score for the weeks before and after starting famotidine, which all showed marked improvements (figure 4B–D).
Patient 9 is a South Asian ex-smoker man in his 50s with history of hyperlipidaemia controlled by rosuvastatin. He took famotidine 60 mg two times daily for 21 days starting 2 days after first experiencing symptoms of COVID-19. He described improvement in his symptoms within 2 days of starting famotidine. He reported possible famotidine associated mild forgetfulness and gastroenterological symptoms that started while he was on famotidine but resolved before he stopped the medication.
Patient 10 is a white former smoker man in his 60s with a BMI of 37.5 without known pre-existing conditions. He took famotidine 20 mg three times daily for 5 days starting 7 days after first experiencing symptoms of COVID-19. He reported a universal improvement in symptoms within the first week of taking famotidine.
Discussion
This case series provides patient-reported outcome measures for 10 consecutively enrolled non-hospitalised patients with COVID-19. They all noticed improvements in their condition in correlation with famotidine use at doses ranging from 60 mg to 240 mg daily. Based on published pharmacokinetic data for famotidine,8 9 we estimate that these treatment regimens would have resulted in peak plasma concentrations of approximately 0.5–2 µM and average plasma concentrations of approximately 0.15–0.7 µM famotidine, assuming normal kidney function. In concordance with the clinical evidence and consensus that famotidine is safe across a wide range of doses and frequencies, famotidine was very well tolerated by all patients. Given that famotidine has only minimal inhibitory effect on the hepatic cytochrome p450 system and low risk of clinically significant alterations in oxidative drug metabolism,10 11 it may be a safe drug for testing in a trial or clinical setting where patients self-administer the medication.
A pertinent aspect of this work is the exploration and application of graded symptom scores and patient-reported outcome measures in tracking COVID-19 in the non-hospitalised setting using a four-point ordinal scale. Using these symptom scores, we were able to determine that all patients noticed a rapid improvement in their condition within 24–48 hours of starting famotidine. Our quantitative approach to follow symptom severity may be a useful tool, in particular for outpatient studies, but requires validation. In addition, for all patients who were able to provide data, temperature readings, oxygen saturations and activity improved in correlation with taking famotidine. These findings suggest that famotidine may affect the course of COVID-19 but must be considered in the context of several limitations. Placebo effect, enrolment bias and recall bias12 for symptoms may affect our findings as is the case for the outcome measures of any non-blinded, non-controlled study, despite us attempting to minimise bias by asking non-leading questions. An improvement of symptoms was noticed within 48 hours by all individuals in this study, despite the symptomatic period prior to taking famotidine varying widely. There remains the possibility, however, that these changes may reflect treatment independent convalescence, as the natural course of COVID-19 in patients who do not require hospital admission is not well characterised.
Our case series suggests, but does not establish, a benefit from famotidine treatment in outpatients with COVID-19. Future work will investigate potential mechanisms of action and clinical relevance of famotidine. Mechanistically, famotidine could have a viral target, for example, one of the viral proteases, or a host target, resulting, for example, in modulation of the immunological response to the virus. Clinically, we unreservedly share the opinion that well designed and informative studies of efficacy are required to evaluate candidate medications for COVID-19 as for other diseases.13 A randomised phase III trial testing the efficacy of high dose intravenous famotidine three times daily in addition to hydroxychloroquine in hospitalised patients with COVID-19 has recently commenced (NCT04370262). An outpatient study of oral famotidine that investigates efficacy for symptom control, viral burden and disease outcome and assesses effects of medication use on long term immunity should be considered to establish if famotidine may be of use in controlling COVID-19 in individual patients while also reducing the risk of SARS-CoV-2 transmission.
Conclusions
The results presented in this case series suggest that high-dose oral famotidine is well tolerated and associated with improved self-reported outcomes in non-hospitalised patients with COVID-19.